Hip Labral Tears: What You Need to Know About Your Hip Pain
If you’re experiencing hip pain, you might be wondering if it’s a symptom of joint damage and a labral tear. Read on to learn what the science says on the correlation between pain and labral tears, how to figure out what may be causing your discomfort, and ways to work toward pain relief.

Table of Contents
- What are Hip Labral Tears?
- How do You Know if You Have a Labral Tear?
- Hip Pain and Labral Tears: The Hidden Truth
- Do Hip Labral Tears Cause Hip Instability?
- What are Treatment Options for Labral Tears?
- Recap: What You Should Do Now
Maybe your doctor has said you have a labral tear in your hip, or maybe you’re experiencing hip pain and wondering if it’s related to a tear. In the age of desk work and constant sitting, these diagnoses are skyrocketing.
In this article, we’ll take a deep look at the research around hip pain, labral tears, when to consider surgery (spoiler: hardly ever), and how functional training can help.
But first, let's define the "enemy."
What are Hip Labral Tears?
A labral tear is conventionally understood as damage to the cartilaginous ring around the hip joint. Orthopedic surgeons may tell you that this lead to catching, clicking, and irreversible damage to the hip joint. They argue that when this cushion deteriorates, it causes arthritis.
[Image of the anatomy of the hip joint showing the acetabular labrum]
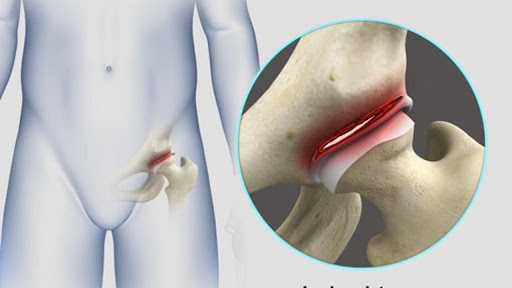
This is what a labral tear looks like.
I have spent years working with clients to navigate these issues, and I've spent too many hours looking into the research (in the age before A.I.!).
My findings have been consistent: The available scientific research and real-world clinical results both indicate that movement—not medical intervention—is the primary path to lasting mobility.
While conventional treatments often focus on the "damage" seen on a scan, a movement-based approach addresses the actual cause of discomfort, preventing the common spiral into further chronic pain.
Tommy's story proves it's possible to heal your hips without surgery.
How do You Know if You Have a Labral Tear?
If you have a positive MRI or MRA, you might think the case is closed. Fix that tear, right?
Not so fast.
The Shocking Reliability of MRI and MRA
Research shows that MRI and MRA have very high false-positive rates. A 2011 study found that MRA had a specificity of only 64 percent. This means if you don't have a tear, your chance of getting a false positive is as high as 36 percent!
Many doctors argue that technology has improved since 2011, but recent research proves the problem is actually getting worse as scanners become more sensitive. Here is what the last decade of science reveals:
- 69% Prevalence in Healthy Hips (2012): Using powerful 3.0-Tesla MRI technology, researchers scanned volunteers with no history of hip pain. They found labral tears in 69% of the joints. (Register et al., 2012)
- Limited Correlation (2015): Research in the Bone & Joint Journal found labral tears in 39% of asymptomatic people, concluding that imaging must be viewed with extreme caution before considering surgery. (Duthon et al., 2015)
- Asymptomatic vs. Symptomatic (2017): A prospective study found that 57% of asymptomatic volunteers had labral or cartilage defects. The study concluded that these findings are common in people without pain and often match the location of defects in patients with pain. (Tresch/Schmitz et al., 2017)
- The "Normal" Athlete (2019): A systematic review and meta-analysis of 5,707 hips found that 54% of asymptomatic athletes (those with NO pain) had labral tears. (Heerey et al., 2019)
Key Takeaway: MRI and MRA can be wrong when they say you have a labrum tear, and they prove nothing about the cause of your hip pain.
The Dismal Reliability of Physical "Special" Tests
A 2010 study examined four common hip maneuvers doctors and physical therapists use to diagnose hip labrum tears. The results? All four were worse than a coin toss.
But doctors will often use multiple tests to be more certain, which should make tests more accurate, right?
Wrong.
Combining multiple tests actually led to a nearly 100% guarantee of a "you've got a tear!" result, even in healthy hips. In other words, if you keep testing a healthy hip with inaccurate tests, you're guaranteed to "prove" someone has a hip labrum tear.
And, no, the very common tests FADIR and FABER aren't accurate either.
Key takeaway: A battery of inaccurate physical tests guarantees you'll be told you have a labrum tear.
The Reliability of Anesthetic Injections
Surgeons often claim that if an anesthetic injection stops your hip pain, you have a labral tear. But a 2008 study found only a 39 percent correlation between pain relief and confirmed tears.
Key takeaway: Injections are not better than a coin toss for diagnosis.
Joint Popping, Snapping, and Clicking and Labral Tears
This is a persistent myth.
The labrum is a soft cushion. Think of it as a slimy little pillow. You cannot make a "snap" or "pop" by rubbing your hand against a slimy little pillow.
Stiff substances—like tendons or bones—make those kinds of sounds. Clicking is far more likely to be a tendon or ligament moving over bone than a soft piece of cartilage "catching."
Hip Pain and Labral Tears: The Hidden Truth
Here is the most important fact in this article: Many people with labral tears have zero pain.
- A 1998 study found the majority of people without pain had tears.
- A 2012 study found a whopping 85 percent of asymptomatic volunteers had labral tears.
- A 2015 study confirmed these findings, noting that tears may just be "normal variations."
- Asymptomatic vs. Symptomatic (2017): A prospective study found that 57% of asymptomatic volunteers had labral or cartilage defects. The study concluded that these findings are common in people without pain and often match the location of defects in patients with pain. (Tresch/Schmitz et al., 2017)
- The "Normal" Athlete (2019): A systematic review and meta-analysis of 5,707 hips found that 54% of asymptomatic athletes (those with NO pain) had labral tears. (Heerey et al., 2019)
Key Takeaway: Having a labral tear doesn't mean you'll have hip pain, and it doesn't mean it's the cause of your hip pain.
Do Hip Labral Tears Cause Hip Instability?
For years, the theory has been that tears cause instability. However, a 2011 cadaver study proved that even big tears did not result in a loss of stability. What did cause instability?
Surgery.
Removing pieces of the labrum (labrectomy) significantly decreased joint stability.
What Are the Treatment Options?
To fix your hip pain, you can try surgery. You can go to a physical therapist and see if their protocol helps. You can try exercises on your own. The process can be frustrating, even if you get surgery.
Let's examine hip surgery first.
Do Surgeries for Hip Labral Tears Work?
One popular surgery, labral debridement (cutting away the "loose" bits), has shown dismal results. This isn't surprising if you remember the cadaver study referenced earlier. A 2014 study showed that nearly half of patients had poor outcomes.
In a stunning display of pro-surgery bias, the study authors proposed that the reason patients got bad results is that the surgeons should have also cut away bone.
It’s like saying, “We tried to fix your flat tire by removing a nail. It didn't work. So we also need to replace the axle and the fender."
Another surgical option, refixation (stitching the labrum), involves puncturing the bone and cartilage to create attachment points. Does adding more holes to a "damaged" joint make sense to you?
The Takeaway: Tissue repair does not equal pain resolution. These studies indicate that if you don't address the muscle imbalances that caused the tear in the first place, the surgery is just a temporary patch. True, long-term satisfaction is built through movement and strength, not a surgeon's stitch.
Why Conventional Physical Therapy Often Fails (And What to Do Instead)
Before diving into PT, we should talk about a highly-cited 2021 study. It claimed surgery was better than physical therapy. That makes physical therapy sound awful and not worth trying at all.
That study was heavily biased. Patients were recruited from surgery clinics and the "physical therapy" group was told not to do strength or flexibility training because they would only get worse. The deck was stacked heavily in favor of the knife.
Watch a full video on this crazy study here.
That said, if you’ve tried physical therapy for a labral tear and didn’t get results, you’re not alone. In major medical trials, "failure" rates for physical therapy are often reported when patients eventually choose surgery. For example, the Mansell et al. (2018) study showed that nearly one-third of patients "failed" PT and opted for the knife. Spoiler: whether you got surgery or not, you ended up with similar long-term outcomes. (Mansell et al., 2018)
But why does PT "fail" so often? Based on my years of clinical experience and a close look at the research, it isn't because the hip is broken—it’s because the protocol is flawed. Here are the three main reasons conventional PT falls short:
- The "Avoidance" Trap: Most PT protocols, like the one used in the UK FASHIoN Trial, focus heavily on avoiding "impingement positions." While this prevents short-term pinching, it stops you from ever building strength and resilience in the ranges of motion you actually use in real life. (Griffin et al., 2018)
- Under-Loading the Muscles: Clamshells with a light band aren't enough. Pelvic tilts and a few planks aren't enough. To make a healthy hip joint, you need to progressively challenge the muscles in ALL the directions, not just one or two. If your PT treats you like you're made of glass, you’ll never gain the stability needed to stop the pain.
- Treating the Scan, Not the Human: Many therapists are just as guilty as surgeons of "treating the MRI." If they believe your pain is caused by a mechanical tear, they won't push the muscular retraining necessary for true recovery.
I made a video that dives deep into why these standard protocols fail. You can watch it here:
To get out of pain, you have to move past the "rest and ice" mentality. You need to focus on strength at every length and trust that your muscles—not a surgeon’s stitch—are the key to a stable hip.
Functional Training Is A Better Way
Retraining your hip muscles can save you thousands of dollars and months of bed rest. Doctors may tell you to "rest and pray," but rest leads to atrophy and decay.
Properly retraining the muscles around the hip can eliminate pain and restore function in a way that surgery simply doesn’t. Always Think Muscles (ATM).
Recap: What You Should Do Now
If you have been told you have a labral tear, keep these points in mind:
- Imaging is unreliable. MRI and MRA have very high false positive rates, and they don't explain your pain.
- Tears don't equal pain. The majority of adults with no hip pain have hip labrum tears in MRI and MRA.
- Muscles move bones. If your hips don't feel good, it could be from the network of hip muscles that are weak, stiff, and deconditioned.
Next Steps:
- Don’t stress! Labral tears are often irrelevant to your symptoms. Focus on function, not the diagnosis.
- Find a therapist or coach who prioritizes movement and form over cookie-cutter templates.
- Establish 3 Habits for Healthy Hips.
- Learn to stretch properly (not aggressively).
- Focus on Muscle Imbalances.
Read more: ATM Theory: Your Joint Pain May Actually be Muscle Pain
Curious about the orthopedic surgery industry? Read: Why you DON’T Need Orthopedic Surgery for Joint Pain

